What the VA’s $13.84B Program Actually Teaches
The U.S. Department of Veterans Affairs (VA) Electronic Health Record Modernization program is the most thoroughly documented EHR failure in history.
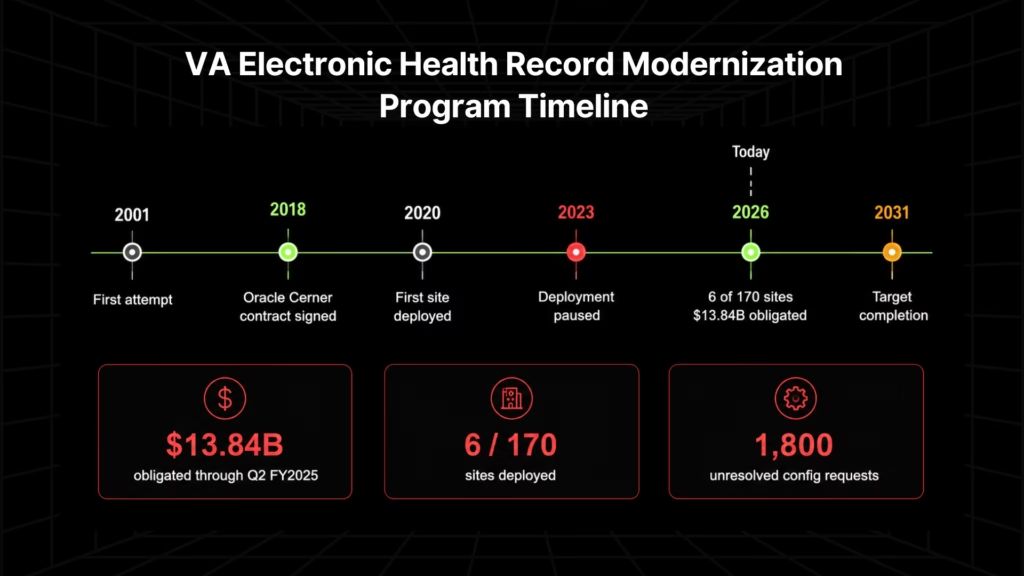
As of April 2026, $13.84B has been obligated, 6 of 170 VA medical centers have been deployed, 1,800 configuration change requests remain unresolved, and full completion is now targeted for 2031, the outcome of four attempts across more than two decades [1].
A GAO survey found that 58% of VA users believed the modernized system increased patient safety risks, and 75% disagreed that it made the VA as efficient as possible [2].
The failure modes are transferable. The dollar figures are federal-scale and do not apply directly to private health systems. But every specific breakdown the GAO documented maps to an execution error that any EHR modernization program can replicate. Five lessons follow.
- Lesson 1: Deploying before clinical logic is extracted guarantees a configuration backlog. The VA’s 1,800 unresolved configuration requests accumulated because the target system was configured before anyone had fully mapped what the legacy system did. Custom order sets, CDS rules, and care pathways built into VistA over decades had no equivalent in the new platform. Private-sector health systems running heavily modified EHR instances on Java EE or .NET Framework carry the same risk at smaller scale.
- Lesson 2: Parity validation is a go-live gate, not a post-go-live cleanup item. The VA documented 14 highest-priority patient safety enhancement requests in March 2023. As of July 2024, only 9 of 14 had been closed, a condition that held the restart of deployments into 2026 [3][4]. Clinical parity is not a QA checkbox. It is the condition under which a system is safe to operate.
- Lesson 3: Security parity requires the full clinical stack, not just the primary EHR. The 2024 Ascension ransomware attack (a Black Basta intrusion through unsupported ancillary servers, not the primary EHR) exposed 5.6M patient records across 140 US hospitals and contributed to a $1.8B operating loss for the fiscal year ended June 2024. Legacy infrastructure running alongside a modernized EHR remains an attack surface. Modernization scope must include it.
- Lesson 4: Interface complexity is always underestimated at the scoping stage. Every EHR connects to 400+ ancillary systems via custom HL7 v2 integrations: lab, pharmacy, radiology, billing, scheduling, medical devices, patient portals, and HIE connections. Each must be rebuilt and revalidated independently. This is consistently the line item that breaks EHR budgets when discovered mid-execution rather than at assessment.
- Lesson 5: Physician adoption failure is a clinical logic problem, not a training problem. When clinical workflows in the new system don’t match the ones physicians built over years in the legacy system, adoption fails. The VA’s 75% dissatisfaction rate is not an outlier. It is the predictable result of deploying a system that doesn’t reflect how the organization’s clinical work actually gets done. The solution is not better training. It is preserving clinical logic through the modernization, so the system physicians receive reflects the system they already know.
This article addresses the EHR application layer: clinical systems running on Java EE, .NET Framework, JSP/Servlets, or VB6. Clinical data migration, EHR vendor selection, and physician adoption program design are adjacent problems not covered here.
Why Legacy EHR Modernization Is Categorically Different: Seven Execution Constraints
Most enterprise application modernization programs carry execution risk. Legacy EHR modernization carries a different category of risk, defined by constraints that either do not exist or do not carry the same consequences in any other application domain.
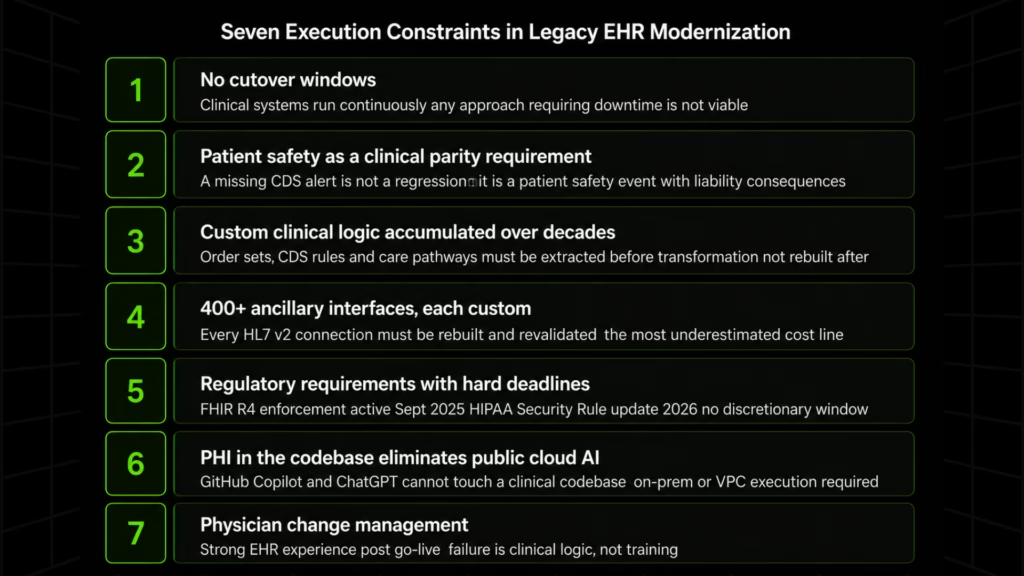
1. No cutover windows
Clinical systems run continuously. Every transformation must execute incrementally while the system is serving active patient care. Any modernization approach that requires a cutover window is not a viable approach for this application type.
2. Patient safety as a clinical parity requirement
A missing clinical decision support (CDS) alert is not a functional regression. It is a potential patient safety event with direct liability consequences. Parity must be confirmed at the clinical output level, not the code level.
3. Custom clinical logic accumulated over decades
Order sets, CDS rules, documentation templates, and care pathways are encoded into the application layer over years of clinical operation. None survives migration without explicit extraction and reconstruction. The VA’s 1,800 unresolved configuration requests are what happens at scale when extraction is skipped [1].
4. 400+ ancillary interfaces, each custom
Every lab system, pharmacy dispenser, radiology PACS/RIS, billing engine, scheduling system, medical device, patient portal, and HIE connection runs on a custom HL7 v2 integration. Each must be rebuilt and individually revalidated. This is the most underestimated cost line in any EHR modernization program.
5. Regulatory requirements with hard enforcement deadlines
| Requirement | Status | Consequence |
| 21st Century Cures Act: FHIR R4 API certification | Enforcement effective September 2025 | Up to $1M per violation (ONC) |
| 2026 HIPAA Security Rule update | Effective 2026 | Encryption at rest and in transit now mandatory |
| Legacy EHRs built before 2015 | Cannot support FHIR natively | Application layer changes required before compliance is achievable |
The regulatory argument for modernization is no longer discretionary for health systems running pre-2015 clinical systems.
6. PHI in the codebase: the constraint that eliminates public cloud AI
Clinical codebases frequently contain protected health information in test fixtures, production-derived development environments, and configuration files. This disqualifies GitHub Copilot, ChatGPT, and generic cloud AI tools from EHR codebase analysis without triggering HIPAA exposure risk.
Any AI-assisted EHR codebase analysis must run on-premises or within a VPC-isolated environment. This is a HIPAA compliance requirement, not a deployment preference.
7. Physician change management as an EHR program risk
Only 18% of physicians report a strong or elite EHR experience after go-live, and the majority dissatisfied at implementation remain dissatisfied more than two years later. Productivity drops of 20 to 40% in the first month are well-documented in US clinical IT literature, with recovery taking 6 to 12 months for organizations without structured optimization programs. These are not soft metrics. They are indicators of whether a clinical program survives politically.
None of these constraints are unique to the VA. Every mid-to-large US health system running a custom-modified EHR on a Java EE or .NET Framework stack carries all seven.
Why Physician Burnout Is an EHR Modernization Problem
Physician burnout is routinely framed as a change management challenge: a problem of training, communication, and transition support. The data suggests a more specific cause.
Physicians using legacy EHR systems spend an average of 2.3 extra administrative hours per day on documentation and workflow tasks compared to those on modern platforms.
In clinical lab workflows, the delay between a critical lab result being generated and a physician taking action averages 4.7 days on legacy EHR systems, compared to 1.2 days on modernized platforms.
These are not usability metrics. They are patient safety indicators tied directly to the technology stack the clinical system runs on.
The standard response is a training and optimization program layered on top of an unchanged system. It does not work. When a physician’s order set workflow, documentation template, or CDS alert configuration does not exist in the modernized system, no amount of training can recover the lost time or clinical logic. The dissatisfaction is structural.
The correct framing should be that physician resistance to EHR modernization is a clinical logic preservation problem. When the modernized system reflects how the organization’s physicians actually practice (because the order sets, CDS rules, and care pathways from the legacy system were extracted and carried through the transformation), adoption resistance drops materially. The training burden is reduced because the system being trained on is recognizable.
Legacy EHR modernization that preserves institutional clinical logic is the same investment that addresses physician burnout at its source. They are not separate programs.
EHR Implementation Cost: What US Health Systems Actually Spend
The choice of the modernization path determines the cost profile. Before comparing paths, a reference frame for real implementation spend across US health systems:
| Organization Size | Typical EHR Implementation Cost |
| Small clinic (1–5 providers) | $500K to $2M |
| Mid-size hospital | $10M to $50M |
| Large health system | $100M to $2B+ |
| VA EHRM program (170 facilities) | $13.84B obligated through Q2 FY2025 |
Disclosed figures from US health system financial reports: Trinity Health $800M across 101 hospitals; Northwell Health $1.2B; AdventHealth $660M; Emory Healthcare $51M (single-system post-acquisition); UK HealthCare $95M. [6]
These figures represent full commercial EHR replacement. Application layer modernization of an existing system operates at a different cost profile, determined by codebase size, interface complexity, and clinical logic volume, not per-bed licensing. The path comparison below maps these differences.
Full Replacement, Phased Modernization, or Application Layer Modernization: Choosing the Right Path
Path 1: Full Commercial EHR Replacement
Epic holds 42.3% of US acute care hospital market share and approximately 54.9% of licensed beds as of 2024. Community Connect captured roughly 70% of all US hospitals involved in EHR decisions in 2024. Full replacement is the dominant commercial path.
What disclosed cost figures do not capture: every custom order set, CDS rule, documentation template, and care pathway must be rebuilt from scratch in the new platform’s configuration environment. The new system’s defaults do not reflect the organization’s clinical workflows. Every ancillary interface must be rebuilt and revalidated. This is the process that produces configuration backlogs, and it applies regardless of which commercial platform is selected.
Best suited for: large US health systems consolidating multiple EHRs post-merger; organizations already in an Epic Community Connect agreement; systems with limited accumulated custom clinical logic.
Path 2: Phased Modernization, FHIR API Layer and Incremental Module Replacement
For US health systems with legacy EHRs built before 2015, FHIR R4 enforcement makes this the compliance-driven path. The FHIR layer serves as the regulatory bridge while transformation runs incrementally beneath it, preserving clinical operations while each module is addressed in sequence.
Each module replacement carries the same clinical logic preservation problem as full replacement, scoped to that module. Interface modernization from HL7 v2 to FHIR R4 is consistently the most underestimated cost line. Discovering the true interface count mid-execution is the most common cause of EHR budget overruns.
Path 3: Application Layer Modernization In Place
For healthcare ISVs modernizing their EHR product stack, and US health systems with heavily modified EHR components where the clinical workflows are the institutional asset and the underlying technology is the liability.
The application layer (Java EE, .NET Framework, VB6, JSP/Servlets) can be modernized to .NET 6/8, Spring Boot, or React without replacing the clinical logic it carries. This is Legacyleap’s terrain. The platform addresses the application layer the clinical system runs on, not the clinical platform itself. It does not compete with Epic or Oracle Health.
Path Comparison
| Factor | Full Replacement | Phased (FHIR + Modules) | Application Layer Modernization |
| Primary driver | Platform consolidation, M&A | FHIR compliance, risk reduction | Technology debt, stack obsolescence |
| Clinical logic | Rebuilt in new platform | Rebuilt module by module | Preserved and carried through modernization |
| Timeline | 18 months to 7+ years | 2 to 5+ years | 6 to 24 months depending on scope |
| Typical cost range | $10M to $2B+ | $5M to $500M+ | Varies by codebase size and complexity |
| Operational risk | High at cutover | Distributed across phases | Managed incrementally |
| FHIR compliance path | Vendor-provided | Explicitly addressed per module | Application layer enablement required |
For US health systems unsure which path is appropriate, the answer depends on what the legacy codebase actually contains. Scoping from documentation alone is the primary cause of EHR budget overruns.
How Legacyleap Executes EHR Application Layer Modernization
EHR modernization programs fail when specific execution stages are skipped, compressed, or sequenced incorrectly. Legacyleap’s five-stage, agent-governed platform addresses each documented failure mode directly, starting with what the system actually contains before changing anything.
Stage 1: Assessment
Programs begin transformation before they understand what’s in the system. The VA’s 1,800 configuration change requests are the public record of what this produces: a replacement system deployed before the legacy system’s clinical logic was mapped [1].
A complete EHR assessment must produce a full dependency map, a clinical logic inventory extracted from the codebase itself, an interface inventory with behavioral specifications for every HL7 v2 connection, PHI presence mapping, and risk stratification by clinical criticality. The path decision cannot be scoped accurately without it.
Legacyleap’s Assessment Agent produces this full inventory, including PHI detection, running entirely within the client’s on-prem or VPC infrastructure. No codebase content is transmitted externally. The assessment output also surfaces the technical debt load that defines legacy EHR maintenance budgets, giving engineering leadership the data to prioritize alongside modernization scope.
Stage 2: Documentation
Organizations discover mid-migration that order sets, CDS rules, and documentation templates that physicians rely on daily have no equivalent in the replacement system.
A peer-reviewed study of EHR transitions found a fivefold increase in medication safety reports in the three months following a clinical system cutover [5]. This is what happens when CDS rules don’t transfer cleanly.
Documentation must produce a clinical logic catalog, interface behavioral documentation, and a validation baseline: the record against which every subsequent transformation stage is tested. Without it, Stage 5 has nothing to measure against.
Legacyleap’s Documentation Agent generates clinical-facing outputs (workflow maps, order set catalogs, care pathway documentation) and technical-facing outputs (API specifications, interface behavioral documentation) from the codebase itself. Clinical validation of the extracted logic is human-owned throughout.
If the clinical logic in your legacy EHR codebase has never been formally extracted, you’re scoping a modernization program without knowing what’s inside it.
A $0 Modernization Assessment produces a dependency and module map, clinical logic risk indicators, interface inventory, and a structured modernization readiness view, derived from your actual codebase, not your documentation. No commitment required.
Stage 3: Recommendation
Architecture decisions made without quantified inputs produce unreliable scopes. Teams choose between refactoring and replatforming on committee consensus rather than actual codebase complexity data. Unrealistic scope, established before anyone ran analysis on the actual system, is the primary cause of EHR budget overruns.
A credible recommendation requires module-level complexity scoring, an interface modernization roadmap, clinical risk sequencing, and dependency ordering.
Legacyleap’s Recommendation Agent generates this roadmap from Assessment and Documentation outputs, producing feasibility scoring, target stack recommendations (.NET 6/8, Spring Boot, React), and sequencing that accounts for clinical risk at each phase boundary.
Stage 4: Transformation
Big-bang transformation creates a divergence problem. By the time the legacy and modernized systems are compared at cutover, clinical edge cases that existed in the legacy system have no corresponding tests in the new one. The VA’s 2023 deployment pause is the documented result [1].
Every transformation in an EHR environment must be incremental, diff-based, and human-reviewable before it touches any component that affects clinical outputs.
Legacyleap’s Modernization Agent operates on a Plan, Execute, Validate, Self-Correct loop. All transformations are diff-based pull requests requiring human review before acceptance. There is no autonomous merging or deployment. See incremental modernization as the only proven approach for systems that cannot go offline.
Stage 5: Validation
Programs validate that the modernized system compiles and passes unit tests. They do not validate that clinical outputs match the legacy system under the full range of patient conditions it was built to handle.
The VA documented 14 highest-priority patient safety enhancement requests as of March 2023; only 9 of 14 were closed before the 2026 deployment restart was permitted [3][4]. This is what validation failure looks like as a go-live gate.
Parity must cover every CDS rule, order set, ancillary interface output, clinical report, and quality measure, tested against legacy behavior, not expected modernized behavior.
Legacyleap’s QA Agent generates the regression safety net from the existing legacy codebase before transformation begins. Parity is validated against what the legacy system actually does. CodeShield scans every AI-generated code block for security vulnerabilities before human review.
Governance Across All Stages
AI cannot make autonomous decisions about clinical systems. Legacyleap’s Governor enforces human approval at every decision point affecting clinical outputs, architectural direction, or release readiness. Every action is logged with a full audit trail.
The ability to demonstrate that no undocumented clinical logic was altered during modernization is a documented HIPAA compliance obligation. The Governor’s audit trail is the evidence that satisfies it.
Healthcare ISV Case Study: JSP and Struts Modernization for a US-based Healthtech Company
This client modernized 300+ JSP screens and 5,000+ Struts forms using Legacyleap, Gen AI, and AWS services. The platform ran entirely within a secure, isolated environment, consistent with the PHI handling requirements that apply to any clinical codebase analysis.
The challenge: A large-scale Java EE frontend built on JSP/Servlets and Struts, carrying years of accumulated clinical workflow logic. Full replacement would have required rebuilding that logic from scratch in a new system. The team needed to modernize the technology stack while preserving the application behavior the clinical users depended on.
How Legacyleap executed it:
- Assessment Agent mapped the full JSP and Struts codebase, including undocumented dependencies and clinical workflow logic
- Documentation Agent generated behavioral specifications for every screen and form, establishing the parity baseline
- Modernization Agent transformed the stack to a modern Angular-based UI incrementally, with all changes as reviewable diffs
- QA Agent validated functional parity against the Documentation baseline before each release
The outcome: A scalable Angular-based UI delivered with documented functional parity to the original system. Reduced downtime, improved user experience, simplified ongoing maintenance, and a codebase no longer dependent on end-of-life Java EE infrastructure.
The full case study is available here: JSP and Struts to Angular Migration for a US HealthTech Company.
EHR Modernization Doesn’t Have to Repeat the VA’s Mistakes
The VA failed not because EHR modernization is technically impossible, but because execution ran out of sequence.
- Transformation preceded comprehension.
- Deployment preceded parity validation.
- Go-live preceded the extraction of the institutional clinical intelligence that the system contained.
Private-sector health systems and healthcare ISVs repeat these failure modes at a smaller scale, with smaller budgets, and with fewer opportunities to recover from a pause.
The five-stage framework above addresses each failure mode directly, with a governed, clinical-logic-aware approach that starts with understanding what’s in the system before changing anything.
Start with a $0 Modernization Assessment. For a legacy EHR codebase, it produces a dependency and module map, clinical logic risk indicators, interface inventory, a modernization blueprint, and effort and timeline ranges, all derived from the actual codebase rather than documentation. Delivered in days. No commitment required.
To see how the agent-governed platform executes at each stage, from assessment through parity validation, book a demo.
FAQs
Costs vary significantly by scope and path. A small clinic typically spends $500K to $2M; a mid-size hospital, $10M to $50M; a large health system, $100M to $2B+. Real disclosed figures: Trinity Health $800M across 101 hospitals, Northwell Health $1.2B, AdventHealth $660M. The VA has obligated $13.84B with 6 of 170 sites deployed. Private-sector programs operate at far smaller scale, but the cost drivers are the same: interface complexity and clinical logic extraction.
A single department typically runs 6 to 12 months. Hospital-wide replacement or modernization: 18 to 36 months. Health system-wide: 3 to 7+ years. The VA contracted an 8-year program in 2018 and is now targeting 2031 after deploying 6 of 170 sites. Timelines are driven primarily by interface complexity, the volume of custom clinical logic requiring extraction and validation, and whether execution is incremental or attempts broad parallel deployment.
EHR replacement means switching to a new commercial platform and rebuilding all clinical logic, order sets, and interfaces in that platform’s environment. Application layer modernization means updating the technology stack the existing system runs on (.NET Framework to .NET 8, Java EE to Spring Boot) while preserving the clinical logic embedded in that code. Legacyleap addresses the latter. The two decisions serve different organizations and are not in competition.
FHIR (Fast Healthcare Interoperability Resources) is the federal API standard for healthcare data exchange under the 21st Century Cures Act. Enforcement of FHIR R4 certification became effective September 2025, with penalties up to $1M per violation. Legacy EHRs built before 2015 cannot support FHIR natively. The application layer must be modified before compliant outputs are achievable. For health systems and ISVs running pre-2015 clinical systems, this is no longer a discretionary argument.
References
[1] Government Accountability Office, VA Electronic Health Record Modernization: Additional Actions Needed to Evaluate Program Performance and Address Risks, December 2025. Figures cited: $13.84B obligated through Q2 FY2025; 6 of 170 sites deployed; 1,800 unresolved complex configuration change requests as of February 2025; 2 of 18 GAO recommendations fully implemented. https://www.gao.gov/products/gao-25-107613
[2] Government Accountability Office, VA Electronic Health Record Modernization: Actions Needed to Address User Satisfaction and Efficiency Concerns, March 2025. 58% of surveyed VA users believed the modernized EHR increased patient safety risks; 75% disagreed the system made the VA as efficient as possible. https://www.gao.gov/products/gao-25-106798
[3] VA Office of Inspector General, Deficiencies in Oracle Cerner EHR Patient Scheduling Contributed to a Veteran’s Death, Report No. 22-00465-95, March 2023. Documents the 2022 death of an Ohio veteran attributed in part to a scheduling error in the modernized EHR system. https://www.oversight.gov/report/VA/Deficiencies-Oracle-Cerner-EHR-Patient-Scheduling-Contributed-Veteran%E2%80%99s-Death
[4] Government Accountability Office, VA Electronic Health Record Modernization: VA Needs to Address Identified Patient Safety Risks Before Resuming Deployments, July 2024. 14 highest-priority patient safety enhancement requests identified; 9 of 14 closed as of July 2024. https://www.gao.gov/products/gao-24-107232
[5] Chabra S. et al., Barcode medication administration and EHR transition: Impact on medication safety event reporting, JAMIA Open, PMC. Fivefold increase in medication safety reports in the three months following an EHR transition at one institution. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8861699/
[6] Diaz N., From $3.8M to $800M: The cost of EHR implementations at 12 hospitals, Becker’s Hospital Review, updated October 27, 2025. Source for Trinity Health ($800M, 101 hospitals), Emory Healthcare ($51M, post-acquisition), and UK HealthCare ($95M) figures.https://www.beckershospitalreview.com/healthcare-information-technology/ehrs/from-15m-to-800m-the-cost-of-ehr-implementations-at-3-hospitals/