Why Legacy Healthcare Systems Have Become HIPAA’s Fastest-Growing Compliance Risk
Healthcare organizations running end-of-life clinical applications sit in a different compliance position than organizations running current systems. The Security Rule was written for systems that receive security updates.
Legacy systems, including EHRs, patient management platforms, and backend claims processors built on .NET Framework 4.x, Java EE, Struts, or VB6, frequently cannot receive them. Patches for critical vulnerabilities are unavailable or would require application reengineering to apply.
The system keeps running because replacing it is expensive and operationally disruptive. The compliance exposure compounds because the regulatory obligation does not suspend for systems that cannot be updated.
Between 2023 and 2025, legacy system failures appeared in OCR enforcement actions with increasing frequency. The pattern is consistent: a known safeguard gap, a documented risk analysis that surfaces it, and no active remediation response.
What that sequence creates is not only a compliance problem. It is the specific factual record that satisfies HIPAA’s willful neglect standard, and the mandatory penalty structure that comes with it.
HIPAA Willful Neglect and the 30-Day Cure Period: Two Separate Mechanisms
HIPAA’s civil penalty structure treats the 30-day cure period as an affirmative defense, a mechanism that can prevent OCR from imposing a penalty at all. Compliance teams often read this as a universal safety net: correct a violation within 30 days and the exposure disappears. That reading is accurate for one category of violations and entirely wrong for another.
Under 45 CFR §160.410, the affirmative defense applies when the violation is not due to willful neglect and is corrected within 30 days of when the covered entity knew or by exercising reasonable diligence, would have known of the violation. For violations that are due to willful neglect, the defense is unavailable. The penalty is mandatory. The 30-day window remains relevant only to determine which mandatory tier applies.
For covered entities and business associates running legacy clinical systems, including EHRs, backend platforms, and administrative applications on .NET Framework, Java EE, Struts, EJB, or VB6, HIPAA legacy system compliance requires understanding this distinction precisely.
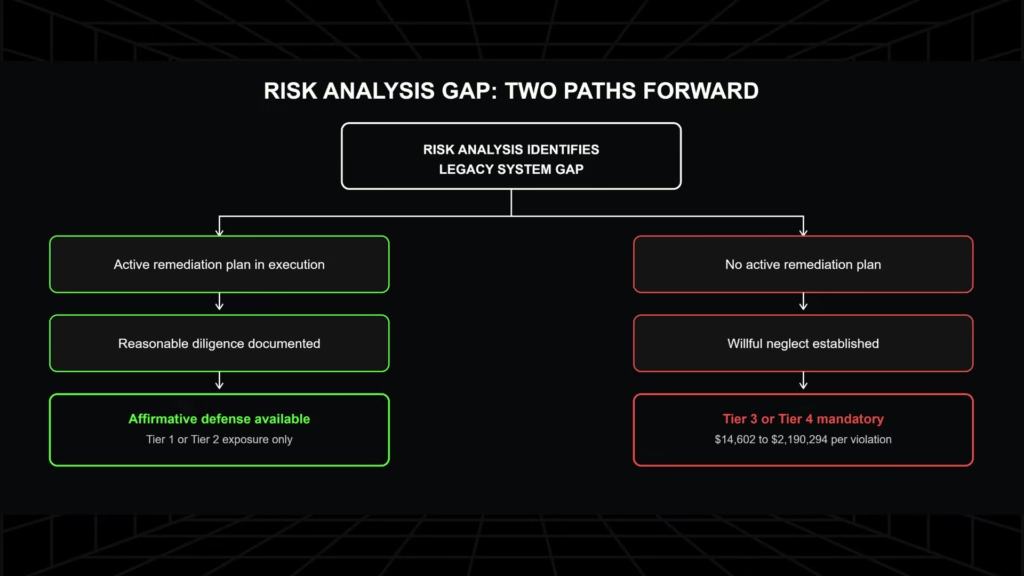
A risk analysis that identifies a safeguard gap on one of these systems, followed by no active remediation plan, creates the exact factual record OCR uses to establish reckless indifference.
The sections below map how that happens, what the diligence record must contain to prevent it, and where Gen AI-assisted modernization fits into building that record fast enough to matter.
HIPAA Penalty Tiers, Willful Neglect, and Criminal Exposure: The 2026 Structure
Two definitions anchor every tier determination that follows, and the penalty amounts, criminal exposure, and enforcement trends in this section all trace back to how those definitions are applied.
Statutory Definitions
The enforcement framework turns on two definitions from 45 CFR §160.401 [1]:
- Willful neglect: “conscious, intentional failure or reckless indifference to the obligation to comply with the administrative simplification provision violated.”
- Reasonable diligence: “the business care and prudence expected from a person seeking to satisfy a legal requirement under similar circumstances.”
These definitions govern tier placement. An organization that knew about a compliance gap and took no action toward resolving it has satisfied the willful neglect definition. An organization that identified the gap, documented it, and took active steps toward remediation has a credible reasonable diligence argument.
How OCR determines willful neglect in practice:
- The organization had actual or constructive knowledge of the compliance gap, established by a prior risk analysis, audit finding, or internal review
- No active remediation plan followed that documentation
- The gap persisted over a meaningful period without compensating controls
- No evidence of diligence exists in the organization’s records at the time of enforcement
The 2026 Civil Penalty Table
OCR adjusts civil monetary penalties annually for inflation. The figures below reflect the January 28, 2026 adjustment [2]:
| Tier | Culpability | Min/Violation | Max/Violation |
| 1 | No knowledge | $145 | $73,011 |
| 2 | Reasonable cause, not willful neglect | $1,461 | $73,011 |
| 3 | Willful neglect, corrected within 30 days | $14,602 | $73,011 |
| 4 | Willful neglect, not corrected within 30 days | $73,011 | $2,190,294 |
Two annual cap regimes exist, and both appear in the literature. The statutory cap across all tiers is $2,190,294 per identical provision per calendar year. A 2019 HHS Notice of Enforcement Discretion set lower annual caps for Tiers 1–3 (ranging from approximately $36,000 to $250,000 inflation-adjusted), which OCR applies “until further notice.”
That notice is not a rulemaking, and OCR can rescind it. When penalty exposure for a multi-year legacy gap is being assessed, the statutory caps are the relevant ceiling because the enforcement-discretion caps apply only to enforcement OCR chooses to bring under them.
Tiers 3 and 4 are both mandatory penalty tiers. Correction timing determines which applies; it does not determine whether a penalty is imposed.
Criminal Penalties: A Separate Track
Criminal enforcement is a DOJ function, independent of OCR’s civil enforcement. The same incident can trigger both simultaneously.
| Track | Enforcer | Applies To | Max Penalty |
| Civil CMPs | OCR / HHS | Covered entities, business associates | $2,190,294/violation |
| Criminal: knowing wrongful access | DOJ | Individuals (employees, ex-employees, contractors) | $50,000 + 1 year |
| Criminal: false pretenses | DOJ | Individuals | $100,000 + 5 years |
| Criminal: commercial gain / malicious harm | DOJ | Individuals | $250,000 + 10 years |
Criminal liability under 42 U.S.C. §1320d-6 attaches to individuals who knowingly obtain or disclose PHI without authorization. The DOJ does not require the individual to know they are violating HIPAA, only that they knew the facts constituting the offense. Employees who access patient records outside their authorization, or who disclose PHI for personal benefit, are within scope regardless of their employer’s civil penalty status.

OCR’s Current Enforcement Posture
OCR launched a dedicated Risk Analysis Initiative in October 2024, and by April 2025 the initiative had produced eight settlements totaling approximately $900,000, all centered on failure to conduct an adequate risk analysis [3].
Enforcement continued through 2025 and into 2026 under both administrations, confirming bipartisan continuity on HIPAA risk analysis compliance. Risk analysis failures appeared in the vast majority of 2025 OCR enforcement actions, a pattern consistent across compliance analysts tracking the initiative.
The initiative’s stated focus was organizations that either failed to conduct any risk analysis or conducted one that was inadequate in scope and failed to drive remediation.
The 30-Day Cure Period Under 45 CFR §160.410: Mechanics and the Hard Boundary
How the Affirmative Defense Works
Section 160.410(c) states that OCR may not impose a civil monetary penalty if the covered entity or business associate establishes that the violation is not due to willful neglect and was corrected within the 30-day period beginning on the first date the entity knew, or by exercising reasonable diligence would have known, that the violation occurred [2].
Three conditions must all be true for the defense to apply:
- The violation is not due to willful neglect
- The correction occurs within 30 days of the trigger date
- The entity can document both the trigger date and the correction
The trigger date matters because it is not the date OCR opens an investigation. It is the date the organization knew or should have known about the violation. A risk analysis that surfaces a security gap sets that date. An audit finding sets that date. An internal security review sets that date. From that point forward, the 30-day window is running against the organization regardless of whether OCR is involved.
The Hard Boundary
The Federal Register enforcement rule is explicit: “violations due to willful neglect are therefore not eligible for extension, nor will their timely correction be an affirmative defense. Timely correction will, however, determine which tier of penalty amounts will be applicable to violations due to willful neglect.” [4]
This means the affirmative defense analysis has a gate. Before assessing whether the 30-day window was met, OCR first determines whether the violation was due to willful neglect. If it was, the gate closes. The defense does not proceed. The only remaining question is whether correction within 30 days limits the exposure to Tier 3 or pushes it into Tier 4.
What Absence of Documentation Costs
Jackson Health System illustrates the consequence of arriving at an enforcement proceeding without a documented diligence record. OCR imposed a $2,154,000 civil monetary penalty in 2019, a CMP rather than a settlement, after investigating HIPAA violations spanning multiple years [5].
OCR explicitly invited Jackson Health to submit written evidence of mitigating factors and affirmative defenses. The system provided no such evidence. OCR determined that the widespread and longstanding extent of the violations, the harm resulting from them, and the poor compliance history left no basis for reduction.
A settlement would have produced a corrective action plan and a negotiated payment. The CMP produced a fixed penalty and no compelled remediation structure. Documentation that could have established diligence was simply not available at the enforcement stage.
For a detailed breakdown of the specific safeguard requirements legacy systems must meet under the current Security Rule, see our HIPAA Security Rule requirements guide for legacy systems.
How a Known Legacy System Gap Becomes a Willful Neglect Finding, and What Prevents It
The mechanism that creates a willful neglect finding and the diligence record that prevents one are two sides of the same fact pattern, starting with how the violation is actually established.
How a Risk Analysis Gap Establishes the Willful Neglect Trigger Date
Consider the scenario OCR’s enforcement posture in 2025 and 2026 is targeting directly. A covered entity operates a clinical application, an EHR, a patient management system, or a backend claims processor, on a legacy stack.
The application may be running on .NET Framework 4.x past its active support window, on Java EE with EJB components, on a Struts-based web layer, or on a VB6 core that predates current encryption standards.
A security risk analysis identifies that the system cannot support multi-factor authentication natively, cannot be patched against a known vulnerability, or cannot produce the audit logs the Security Rule requires.
The risk analysis finding is documented. No active remediation plan follows.
Under 45 CFR §160.401, that sequence establishes the trigger date. The organization now “knew or by exercising reasonable diligence would have known” of the violation. The documented gap without a responding action plan is the factual record that satisfies “reckless indifference to the obligation to comply.” The affirmative defense is unavailable for what follows.
OCR’s January 2026 cybersecurity newsletter confirmed this directly. The Security Rule risk analysis provision applies to all ePHI environments, including legacy systems. Where patches are unavailable, which is the structural reality for end-of-life applications, the obligation to assess, document, and take compensating action remains [6]. The obligation does not suspend because replacement is difficult or expensive.
OCR’s 2026 enforcement posture moved from asking whether organizations identified their gaps to asking whether they acted on them. A risk analysis that surfaces a legacy system’s safeguard failures and sits unresponded to is not evidence of diligence.
For a full accounting of what staying on legacy infrastructure costs beyond the penalty exposure, see our analysis of the total cost of maintaining legacy systems.
What Reasonable Diligence Requires for a Legacy System That Cannot Be Immediately Replaced
The statutory standard is not perfect compliance on a fixed date. It is “the business care and prudence expected from a person seeking to satisfy a legal requirement under similar circumstances.” Immediate replacement of a mission-critical clinical system is often not feasible within a 30-day window. OCR’s enforcement record acknowledges this.
What OCR requires is evidence that the organization is behaving like a prudent actor: identifying the gap precisely, taking interim steps, and executing a credible plan toward resolution.
Four elements appear consistently in the enforcement record as constituting that standard for a known legacy gap:
- Risk analysis: A current, thorough risk analysis naming the specific safeguard the legacy system cannot meet, with the ePHI scope it affects
- ePHI data-flow map: Shows exactly where the exposure exists, which systems touch which data, and through which pathways
- Compensating controls: Documented at the infrastructure layer where feasible: network segmentation, access proxies enforcing MFA at the gateway, storage-layer encryption where native encryption is unavailable, with explicit documentation of what each control does and does not close
- Active remediation plan: Defined scope, phased timeline, and accountable owners. A future-dated intention is not sufficient; the plan must be producing artifacts and demonstrably in execution
OCR has stated directly that migration plans submitted under legacy exceptions will be scrutinized for credibility in enforcement proceedings. A plan dated well before an OCR inquiry and visibly in progress carries weight. A plan drafted after a breach notification does not.
If your risk analysis has identified a legacy system gap with no current remediation plan behind it, the diligence record does not yet exist. Legacyleap’s $0 Modernization Assessment produces the technology asset inventory, ePHI data-flow map, and ordered remediation roadmap, running entirely inside your infrastructure, in 3–5 days. Claim your $0 Assessment.
How Legacyleap’s Gen AI-Assisted Modernization Produces the Diligence Artifacts OCR Looks For
The diligence record this article has described is not abstract. It is a specific set of artifacts: a current risk analysis naming the exact safeguard gap, an ePHI data-flow map, documented compensating controls, and an active remediation plan in execution.
Producing all four manually, for a system with no current documentation, is the reason most organizations end up with a stale risk analysis instead of a credible one.
Legacyleap is a US-based Gen AI-powered legacy application modernization platform built on multi-agent orchestration. Its Legacy System Security Assessment maps a legacy estate’s vulnerabilities, patch gaps, and compliance risk directly against the codebase, rather than against vendor documentation that may no longer reflect what the system actually does.
What the Assessment Produces
| Deliverable | What It Establishes for the Diligence Record |
| Security debt inventory | Every finding by file, type, and severity, the specific record of what the system cannot meet |
| Fix approach per finding | What was found and what remediation each finding requires |
| Modernization opportunity map | Where the system’s architecture allows targeted remediation versus full replacement |
| Go-forward recommendation | A phased plan with defined scope, the active remediation roadmap OCR looks for |
| Post-modernization security validation | Evidence the remediation was executed, not just proposed |
The assessment runs entirely inside the organization’s own infrastructure. No source code leaves the environment at any point. Findings are delivered in 3 to 5 days, which is fast enough for the diligence record to exist before an audit cycle closes rather than after a breach forces the issue.
Why Codebase-Level Mapping Matters for ePHI Exposure
A risk analysis built on outdated architecture diagrams or institutional memory cannot reliably identify where ePHI actually flows through a legacy system. Gen AI-assisted analysis reads the codebase directly: module boundaries, data-flow paths, dependency chains, and the specific points where a safeguard such as encryption at rest or audit logging is structurally absent.
That output is the ePHI data-flow map and technology asset inventory a credible risk analysis requires, generated from what the system does rather than from what someone remembers it was built to do.
Once findings are mapped, the same platform can execute the remediation. Diff-based, human-reviewed code changes carry the fix through to production, and automated regression validation confirms the modernized system performs identically before deployment. The result is a documented chain from finding to fix, the exact evidence an active remediation plan is supposed to leave behind.
For coverage of how clinical systems modernization intersects with FHIR R4 readiness and HIPAA compliance, see our healthcare application modernization guide.
The Compliance Case for Documentation That Precedes the Investigation
A covered entity running a legacy system it knows cannot meet a required HIPAA safeguard, without an active remediation plan in execution, has already satisfied the factual conditions for a willful neglect finding. The 30-day cure period will not erase that liability. It will determine whether the mandatory penalty lands at Tier 3 or Tier 4.
The protection is not a faster correction after OCR makes contact. It is the documented record, a current risk analysis, ePHI data-flow map, compensating controls, and an active remediation plan, that demonstrates the organization exercised the business care and prudence a legal obligation requires. That record needs to exist before the investigation opens, not in response to it.
Book a Legacy System Security Assessment. Legacyleap maps the CVEs, patch gaps, and compliance risk inside your legacy estate and delivers a phased remediation plan, entirely inside your infrastructure, with findings in 3 to 5 days.
If you want to see how the platform works against a specific legacy healthcare stack before sharing code, book a technical demo.
FAQs
Yes. Under 45 CFR §160.402, OCR can impose civil monetary penalties directly on business associates, including mandatory willful neglect penalties, on the same four-tier terms as covered entities.
It can mitigate penalty amounts and CAP duration, but it does not eliminate them. The safe harbor applies only if a recognized security framework such as NIST has been actively implemented for at least the preceding 12 months.
Yes. The annual cap applies per identical violation per calendar year. A Tier 4 willful neglect violation persisting across three years carries up to $6,570,882 in potential exposure under the statutory cap.
Not civilly, but yes criminally. Individual employees face personal criminal exposure under 42 U.S.C. §1320d-6 if they knowingly access or disclose PHI outside their authorization, independent of the organization’s civil penalty.
No. The window starts on the date the organization first knew or should have known of the violation. A third-party audit does not reset that date for gaps the organization had prior knowledge of.
References
[1] 45 CFR §160.401. Definitions (willful neglect, reasonable diligence, reasonable cause). Cornell Legal Information Institute. https://www.law.cornell.edu/cfr/text/45/160.401
[2] 45 CFR §160.410. Affirmative defenses. Cornell LII. https://www.law.cornell.edu/cfr/text/45/160.410
[3] HIPAA Journal. 2025 Healthcare Data Breach Report. https://www.hipaajournal.com/2025-healthcare-data-breach-report/
[4] Federal Register, October 30, 2009. HIPAA Administrative Simplification: Enforcement. https://www.federalregister.gov/documents/2009/10/30/E9-26203/hipaa-administrative-simplification-enforcement
[5] HHS Office for Civil Rights. OCR Imposes $2.15 Million Civil Money Penalty Against Jackson Health System. October 23, 2019. https://www.hhs.gov/hipaa/for-professionals/compliance-enforcement/agreements/jackson/index.html
[6] HHS OCR Cybersecurity Newsletter, January 2026. https://www.hhs.gov/hipaa/for-professionals/security/guidance/cybersecurity-newsletter-january-2026/index.html
[7] Federal Register, January 28, 2026. 2026 HIPAA Civil Monetary Penalty Inflation Adjustment. https://www.govinfo.gov/content/pkg/FR-2026-01-28/pdf/2026-01688.pdf