The Real Cost of Outdated Patient Scheduling Software
Patient scheduling software modernization has attracted more investment in the last five years than almost any other operational category in US healthcare. Self-scheduling portals, AI-assisted booking engines, automated reminder systems, etc., the tooling has improved substantially. The outcomes have not.
No-shows cost US healthcare approximately $150 billion annually, with each missed appointment averaging $200 in lost revenue and a 23% average no-show rate across specialties [2].
The average wait time for a new patient appointment reached 31 days in 2025, up 19% since 2022 and 48% since 2004, measured across 1,391 physician offices in 15 major US metros [1].
The demand for better scheduling is not a marginal preference. The majority of patients say 24/7 digital scheduling matters to them, and a significant share would change providers to get it. Yet digital self-scheduling adoption at most practices remains low. The demand exists. The investment has moved. The gap keeps widening.
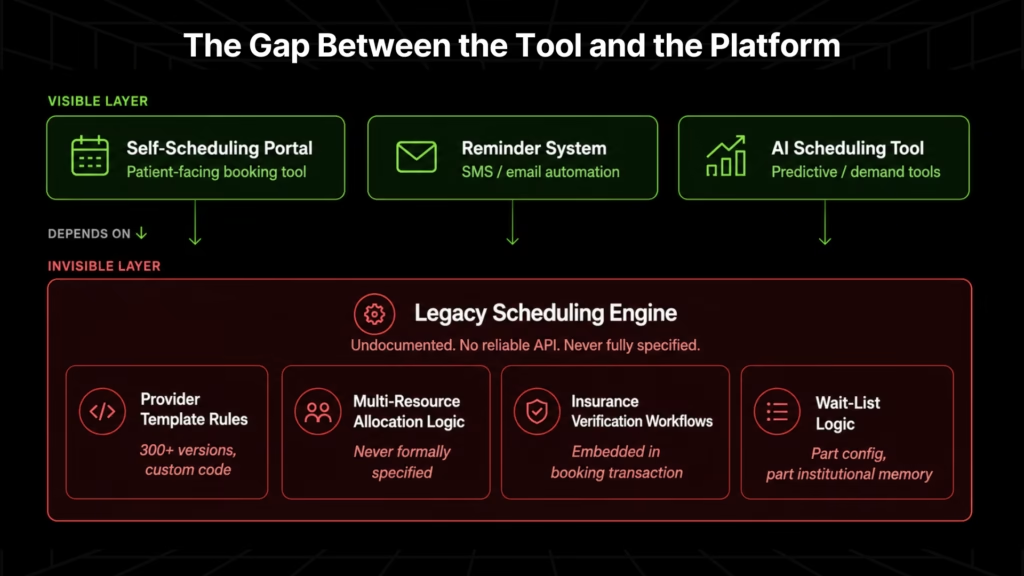
The question the data raises is why. The answer is not the front-end tool. It is the platform underneath it.
Why Off-the-Shelf Patient Scheduling Software Cannot Handle Enterprise Complexity
The first response from most health system IT teams is to evaluate commercial scheduling platforms: Zocdoc, NexHealth, Epic Cadence, or one of a dozen scheduling-adjacent tools marketed to healthcare.
These tools work well in the environments they were designed for, such as practices with a small number of providers, standard appointment types, and clean availability data.
Enterprise health systems are not those environments. A system managing 200-plus providers has provider templates, multi-resource allocation rules, embedded insurance verification logic, and wait-list workflows that no commercial scheduling product replicates out of the box.
The configuration options these tools offer assume that availability data is structured and queryable. In most legacy scheduling platforms, it is not. It exists as custom logic built and modified over years, visible only in the codebase.
This is a comprehension problem, because the logic that governs how appointments are booked, confirmed, and managed at enterprise scale lives in code that has never been fully documented. No off-the-shelf vendor can read it, and no implementation team can configure against what they cannot see.
Why Scheduling Upgrades Always Break at the Legacy Platform Layer
Health systems have funded three distinct waves of scheduling modernization over the past decade. Each one stalls at the same point because the platform it needs to connect to has never been documented.
Self-Scheduling Overlays
Self-scheduling depends on one thing the legacy scheduling engine rarely delivers: accurate, real-time provider availability through a reliable API. Most enterprise scheduling platforms were not built to expose this data.
Provider templates such as the rules governing which appointment types a provider accepts, in which locations, during which clinic sessions, and with which insurance restrictions, live inside the scheduling engine as custom logic, not as structured, queryable data.
When a self-scheduling overlay queries the system, it receives stale data, incomplete availability windows, or nothing usable at all. Patients book slots that are already taken. Providers appear unavailable when they have openings. Staff spend the first hour of every clinic session manually correcting what the portal produced.
MGMA’s July 2025 survey of practice managers explicitly names “EHR integration gaps and outdated scheduling platforms” as the primary operational blocker to self-scheduling adoption. Not patient reluctance, not tool quality, not configuration choices [3].
Automated Reminder Systems
SMS-based appointment reminders work. A systematic meta-analysis found that SMS reminders reduce no-show rates by 38% on average [4]. The mechanism is established. The failure point is upstream.
Reminder systems depend on accurate scheduling data:
- the right provider name,
- the correct appointment time,
- the right location.
Legacy platforms that export appointment data via flat-file batch processes introduce lag, formatting inconsistencies, and mismatched fields. A reminder that fires with the wrong clinic location or a provider name that doesn’t match the patient’s expectation generate a call to the scheduling desk.
At scale, staff exception-management of reminder failures consumes more time than the reminders save.
AI Scheduling Tools
Predictive no-show scoring, demand forecasting, and dynamic slot allocation all require the same input: structured historical appointment data with consistent, queryable fields across appointment types, providers, specialties, and payer categories.
Legacy scheduling platforms that cannot generate a basic provider utilization report by appointment type cannot feed a machine learning model. The AI layer does not fix the data problem. It makes the data problem impossible to ignore.
The Common Failure Pattern
| Scheduling Investment | What It Requires | What the Legacy Platform Provides | Result |
| Self-scheduling overlay | Real-time provider availability via API | Batch exports; no reliable API surface | Stale data; incorrect availability; patient-facing errors |
| Automated reminders | Accurate appointment data: provider, time, location | Inconsistent flat-file exports; field mismatches | Reminder failures; staff exception-management; no net time savings |
| AI scheduling / predictive no-show | Structured historical data with consistent schema | Undocumented schema; no consistent appointment taxonomy | Model cannot train; AI layer stalls at data prep |
| EHR, billing, or patient portal integration | Documented API or data contract from the scheduling engine | No documented interface; integration points exist only in code | Each integration is custom, fragile, and breaks on platform changes |
Every initiative fails at the same structural point: the legacy scheduling platform’s logic has never been documented, so nothing can reliably connect to it, replace it, or build on top of it.
If your scheduling environment matches any of the patterns above, the first diagnostic step is a complete picture of what your current platform actually contains. Legacyleap’s $0 Scheduling Assessment maps your provider template logic, resource allocation rules, and integration dependencies in 3 to 5 days. No project commitment required.
Request your assessment to see what is inside your scheduling system before any platform decision is made.
The Undocumented Logic That Makes Enterprise Scheduling Hard to Replace
Enterprise scheduling platforms are not configuration tools. They are custom rules engines built over years of provider-operations negotiation, modified incrementally by scheduling coordinators and IT staff, and documented (where documented at all) in ways that no longer reflect what the system does. Understanding what is inside them is the prerequisite for changing anything safely.
Provider Template Logic
Every provider in an enterprise health system has a scheduling template. That template encodes availability rules, appointment types and durations, room requirements, staff dependencies, insurance restrictions, new-versus-return patient ratios, clinic session structures, and overbooking parameters by appointment type and day of week.
A system with 300 providers has 300 versions of this complexity, each built over years and modified dozens of times.
A single provider template at a mid-sized academic medical center might contain:
- 48-week availability rules across two clinic locations
- 14 distinct appointment types with different durations and room assignments
- Insurance-specific slot reservations across three payer categories
- New-to-return patient ratios enforced by session and by day of the week
- Manual overbooking allowances by appointment type
- Academic half-day exceptions on a 12-week cycle
That logic exists in code. Scheduling coordinators understand it operationally. IT staff have modified it on request without always understanding the downstream effects. The system’s own documentation, where it exists, was accurate when written and has not kept pace with the changes made since.
Multi-Resource Allocation
Enterprise scheduling does not book a provider. It simultaneously books a provider, a room, equipment, and support staff within the same time window, subject to constraints that interact in ways that have never been formally specified.
An infusion appointment requires an oncologist, a specific chair in the infusion suite, an IV pump, a chemotherapy-trained nurse, and pharmacy pre-authorization, all resolved in the same scheduling transaction.
A cardiac stress test requires a cardiologist, a treadmill room, an ECG technician, and verified eligibility before the slot is confirmed. This logic is custom code refined through years of operational problem-solving. No off-the-shelf scheduling tool replicates it without a full specification of the constraints, and that specification does not exist in any document.
Insurance Verification Workflows
Eligibility checks, referral validation, and pre-authorization rules vary by payer, specialty, procedure type, and sometimes by individual provider contract. These rules run during the booking transaction and determine whether a slot can be confirmed. They are not a separate module but are embedded in the scheduling flow itself.
Front-end scheduling issues account for 32.5% of total claim denials [5]. When insurance verification logic embedded in the scheduling engine is outdated because a payer contract changed, a new procedure code was added, or a referral requirement was modified, the failure surfaces weeks later in the revenue cycle.
By the time the denial arrives, there is no record of what the system told the scheduling coordinator at the point of booking.
Wait-List Logic and Institutional Knowledge
Every large scheduling operation has a wait-list management process that is partly in the system and partly not.
Urgency classifications, auto-fill triggers, notification rules, and cancellation-response workflows are typically a combination of configured system logic and manual workarounds maintained in spreadsheets and carried in the operational memory of experienced scheduling coordinators.
When those coordinators leave, or when the platform is replaced, that institutional knowledge does not transfer. The modernization project discovers its absence six months after go-live, when wait-list behavior stops matching what operations expected.
| Scheduling Logic Component | Where It Lives | Risk if Undocumented |
| Provider template rules | Custom code in scheduling engine | Replacement platform cannot replicate provider availability correctly |
| Multi-resource allocation constraints | Custom transaction logic | Double-booking; resource conflicts; appointment type errors post-migration |
| Insurance verification workflows | Embedded in booking transaction | Claim denials increase; revenue cycle impact appears weeks after scheduling |
| Wait-list and urgency logic | Partial system config; partial institutional knowledge | Wait-list behavior breaks post-migration; staff escalation load increases |
| EHR and billing integration points | Undocumented API calls in code | Integrations break on platform changes; no documented interface to rebuild from |
Scheduling systems are tightly coupled to EHR, billing, insurance verification, and patient portal infrastructure in ways that only become visible when the code is read directly. That coupling is why every attempt to replace or upgrade a scheduling platform without a full comprehension phase produces the same result: partial functionality, integration failures, and a rollback.
How Legacyleap Addresses the Comprehension Problem
The three sections above point to a single prerequisite: the current scheduling platform’s logic must be extracted from the code before anything else can be done safely. It needs to be read from the code itself and converted into a specification that the organization can review and act on.
That is what Legacyleap’s Assessment Agent and Documentation Agent do.
Assessment Agent
The Assessment Agent reads the legacy scheduling codebase at the system level, extracting provider template rules, multi-resource allocation logic, insurance verification workflows, and wait-list algorithms from undocumented code.
It produces a dependency map showing how scheduling logic connects to EHR, billing, and patient portal systems, along with risk indicators for each component and a structured modernization readiness view.
This is the entry point for a $0 Assessment. It does not require a project commitment or a platform decision. It answers the question the organization does not currently have an answer for: what does this system actually contain?
Documentation Agent
The Documentation Agent converts that comprehension into a readable, reviewable business rule catalog. Every provider template constraint, every resource allocation rule, every insurance verification workflow, every wait-list trigger, in a form that scheduling operations leadership can review and that a modernization team can build against.
This catalog is the specification that makes safe modernization possible. Without it, any project is scoped against incomplete information. With it, every platform decision is grounded in what the system actually does.
QA Agent
The QA Agent validates that the modernized scheduling platform produces behavior identical to the original before go-live. Parity is verified through behavioral comparison, not assumed through configuration review.
This closes the most common failure mode in scheduling modernization: a technically complete migration that breaks operationally because the new platform handles edge cases differently from the original.
Financial Impact of Scheduling Modernization
Scheduling modernization is not an IT infrastructure expense. It is the prerequisite for every revenue recovery initiative already on the health system’s roadmap. Three financial levers become available once the comprehension phase is complete and the platform is modernized.
- Self-scheduling adoption. A scheduling platform that exposes accurate, real-time provider availability through a documented API enables self-scheduling to function as designed. One practice that resolved the underlying scheduling data layer before deploying self-scheduling saw inbound scheduling calls drop 60% and appointment volume increase 23% with no added provider hours. The capacity existed. The booking channel was not reliable enough to reach it.
- No-show reduction. Reminders reduce no-shows by 29 to 38% when the scheduling data feeding them is accurate [4]. Against a $200-per-slot baseline at enterprise scale, even a modest improvement in no-show rates produces material revenue recovery. The mechanism works. The data layer is the blocker. Modernization removes it.
- AI scheduling viability. Predictive no-show scoring and demand forecasting require structured appointment history in a consistent, queryable form. That structure is a direct output of scheduling platform modernization. The AI layer does not create it. Understanding this reframes the investment: $150 billion in annual no-show costs is scheduling technical debt made measurable, and the AI tools already budgeted for are waiting on the same fix.
- Revenue cycle recovery. Front-end scheduling issues account for 32.5% of total claim denials [5]. When insurance verification logic embedded in the scheduling engine is outdated, the failure surfaces in the revenue cycle weeks after the appointment, long after the scheduling transaction that caused it. A modernized scheduling platform with documented, current insurance verification workflows closes this loop at the point of booking, not at the point of denial. For health systems processing thousands of claims monthly, the denial rate improvement from accurate scheduling-side verification is measurable within the first billing cycle.
The question facing most health systems is not whether to modernize. It is whether to proceed with a complete understanding of what the platform contains, or without one. Projects that skip the comprehension phase produce predictable outcomes: integration failures, operational exceptions, partial rollbacks, and a second project to correct the first.
For scheduling systems that cannot go offline during migration, the incremental path is available once the business rule catalog exists. Without it, there is no basis for scoping what incremental means.
Read more: Incremental Modernization Strategies for Enterprise Legacy Systems.
Start with a $0 Modernization Assessment for a complete dependency map, scheduling business rule catalog, and modernization readiness view for your scheduling platform, before any project scope is committed.
Book a Demo to see how Legacyleap extracts and documents legacy scheduling logic at the system level.
FAQs
No-shows cost US healthcare approximately $150 billion annually, with a 23% average rate across specialties and $200 in lost revenue per missed appointment [2]. The scale of the number is not the useful insight. The useful one is that no-show reduction tools (reminders, predictive scoring, waitlist automation) all depend on scheduling data that most legacy platforms cannot deliver cleanly. The financial exposure is structural, not behavioral.
The average wait time for a new patient appointment reached 31 days in 2025, up 19% since 2022, across 1,391 physician offices in 15 major US metros [1]. Most health systems have the capacity to schedule faster. The constraint is a scheduling platform that cannot surface accurate, real-time availability to the channels patients and staff are trying to use. Wait time is an access problem with a scheduling data root cause.
The majority of patients say the ability to book online or via mobile matters when choosing a provider, and a significant share would switch providers to get it. The adoption gap at most health systems is not patient reluctance. It is a scheduling platform that cannot deliver consistent, accurate availability data to a self-scheduling layer. The demand has been there for years. The platform has been the constraint.
The technical answer: self-scheduling requires real-time provider availability through a reliable API, and most legacy enterprise scheduling platforms were not built to expose this. Provider templates, insurance restrictions, and multi-resource constraints exist as custom code, not structured queryable data. The practical answer: the self-scheduling tool is not the problem. The platform it depends on has never been documented well enough to support it.
A provider template encodes each physician’s scheduling rules: availability windows, appointment types and durations, room requirements, insurance restrictions, new-versus-return patient ratios, and overbooking parameters. These rules exist in the scheduling system’s code, not in any document. A health system with 200 providers has 200 distinct versions of this complexity, each modified over years. Any migration or integration project that does not begin by extracting and documenting this logic is scoping against an incomplete picture of what the system does.
References
[1] AMN Healthcare. 2025 Survey of Physician Appointment Wait Times. Covers 1,391 physician offices across 15 major US metros. https://www.amnhealthcare.com/amn-insights/physician/surveys-white-papers/2025-physician-wait-time-survey/
[2] Sánchez-Llorens et al. No-show rates and associated factors in outpatient specialty care. Frontiers in Digital Health, 2025. https://www.frontiersin.org/articles/10.3389/fdgth.2025.1543998
[3] MGMA Stat. Majority of medical group leaders report scheduling technology gaps as primary barrier to self-scheduling adoption. July 2025. https://www.mgma.com/mgma-stat/mgma-stat-majority-of-medical-group-leaders-say-their-organizations-are-making-investments-to-reduce-patient-wait-times
[4] Boksmati N, et al. The effectiveness of SMS text message reminders on reducing missed medical appointments: a systematic review. Journal of Telemedicine and Telecare, 2016. https://journals.sagepub.com/doi/10.1177/1357633X16648701
[5] SSI Group. 2024 Claim Denial Benchmarking Report. Front-end scheduling issues account for 32.5% of total claim denials. https://www.thessigroup.com/resources/2024-claim-denial-report/