Legacy RCM Systems Are Leaking Revenue Your Organization Has Already Earned
At 3 to 5% net revenue leakage, a $500M health system is losing $15 to $25M annually to billing inefficiencies a modernized RCM platform directly addresses. At a 1.3% median adjusted operating margin, that is not a performance gap. It is an existential one.
US hospitals lost $48.4 billion in billable revenue in 2025, revenue for care delivered and never collected [1]. Net revenue leakage was up 25% year-over-year, driven primarily by clinical denials for lack of prior authorizations and medical necessity. More than 41% of providers are now running above a 10% denial rate.
The instinctive diagnosis is payer aggression. Medicare Advantage denial rates sit at more than double the rate for traditional Medicare, and the gap is widening. A peer-reviewed study published in npj Digital Medicine in February 2026 found that MA denial rates increased significantly following expanded AI deployment by major insurers [3]. Payers are automating the front line of claims adjudication. That pressure is real and accelerating.
But the more consequential problem is on the provider side. The billing infrastructure processing every claim was built incrementally over 15 years by billing specialists responding to payer policy changes, coding updates, and contract renegotiations. Most of that logic was never documented. Much of it lives only in the people who built it, the majority of whom are no longer at the organization.
This is the problem that RCM system modernization must solve. Before any path forward is viable, whether platform replacement, AI overlay, or comprehensive transformation, the financial logic inside the billing system has to be understood. Everything else follows from that prerequisite.
Why Legacy Billing Systems Create a Different Category of Modernization Risk
Every enterprise modernization project carries technical risk. RCM modernization carries a different category of risk, defined by two structural properties no other application type shares.
Property 1: Embedded, Undocumented Financial Logic
Claim scrubbing rules are the most financially consequential code in a US provider organization’s technology estate. They encode payer-specific validation requirements, NCCI edits, ICD-10/CPT combination rules, modifier logic, LCD/NCD applicability, and prior authorization tracking. This is the logic that governs whether a claim reaches the payer in a billable state or triggers an immediate denial.
This logic was not designed by an IT team with version control discipline. It was built piecemeal by billing specialists responding to payer policy changes, each adding a rule, adjusting a threshold, or hardcoding an exception.
Commercial scrubber vendors acknowledge a “black box” dynamic: errors go in, alerts come out, and the underlying ruleset is rarely fully visible even to the people operating it. When the scrubber is embedded in a legacy platform rather than a standalone product, that opacity compounds significantly.
The people who built these rules have largely moved on. No documentation was produced because there was no formal requirement to produce it. The logic exists in code and in institutional memory that is no longer reliably available.
RCM connects EHR, scheduling, pharmacy, lab, clearinghouse, and payers, making it among the most financially tightly coupled systems in any enterprise. Touching one layer without a complete map of the others produces failures that are not immediately visible and are expensive to reverse.
Property 2: Zero Error Tolerance
In an ERP modernization, a regression creates rework. In a reporting system, a logic error produces inaccurate dashboards. Both are recoverable internally. RCM failures do not stay internal.
A billing rule that migrates incorrectly sends a wrong claim to the payer. Timely filing windows, typically 60 to 365 days depending on payer contract, begin the moment the claim should have been filed. If the error is not caught and resubmitted within that window, the revenue is permanently lost. No recovery mechanism. No appeal pathway.
This makes the zero-error-tolerance constraint governing billing system modernization categorically different from anything else in the enterprise modernization portfolio. “Ship and fix” is not a viable strategy in RCM. Parity must be validated before go-live, not discovered after.
The Cash Flow and Regulatory Constraints
Claim submission continuity cannot be interrupted. US provider organizations operating at 1.3% median margins cannot absorb even a partial disruption to their claim pipeline without creating liquidity gaps that stress operations within weeks.
Large health system platform replacements routinely run 12 to 24 months, an extended period during which the legacy system must remain fully operational and claims must continue to flow without interruption.
CMS-0057-F, effective January 1, 2026, established 7-calendar-day standard prior authorization decision timelines and a 72-hour urgent timeline [4]. FHIR API compliance is required by January 2027. Legacy RCM systems were not built with real-time PA tracking or FHIR-compatible interfaces.
Meeting these deadlines requires architectural changes that most legacy platforms cannot accommodate incrementally.
The Architecture Lesson From Change Healthcare
The Change Healthcare breach produced $2.87 billion in total financial impact. It caused 80% of US physician practices to lose revenue and required $8.9 billion in emergency advances to providers [5]. The scale of disruption was not a function of the breach alone. It was a function of architecture.
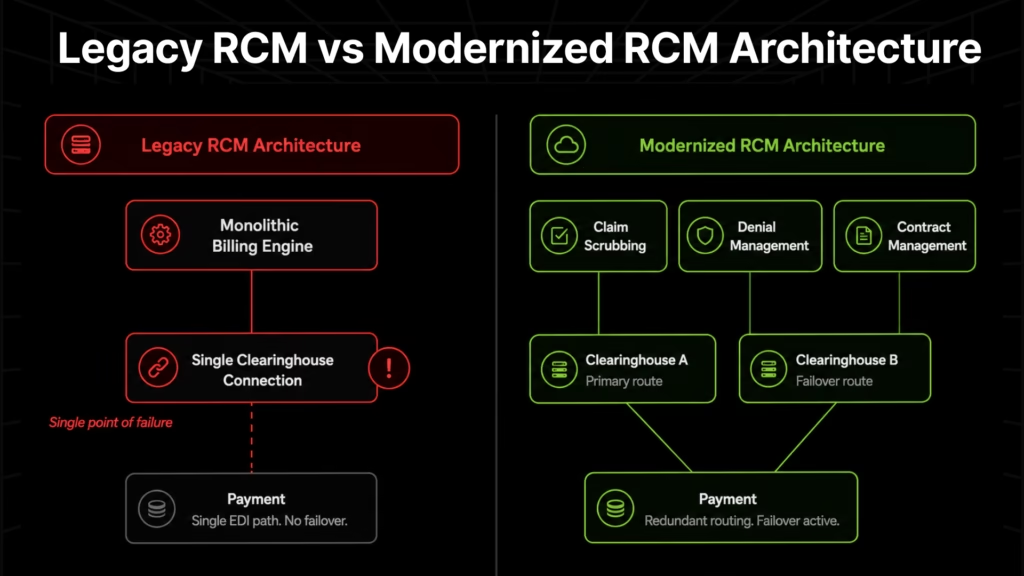
Change Healthcare operated as a centralized clearinghouse with single-source integrations. When the system went down, the entire claim pipeline stopped. Providers had no redundancy, no failover, and no alternative routing.
Most legacy RCM platforms carry identical architecture patterns: centralized EDI connections, single-vendor clearinghouse dependencies, no redundant pathways. The October 2025 TriZetto breach, where attackers maintained access for nearly a year before detection affecting more than 44 HIPAA-covered entities, reinforced the same point. Single-point-of-failure RCM architecture is a demonstrated vulnerability, not a theoretical one.
Where 15 Years of Billing Logic Hides in Your RCM System
Legacy RCM billing logic does not accumulate randomly. It concentrates on specific components, each one a site where undocumented rules have compounded over time, and each one carrying a specific revenue risk if that logic is lost or incorrectly migrated.
| Component | Where Legacy Logic Accumulates | Revenue Risk If Logic Is Lost |
| Claim scrubbing rules | Payer-specific validation, NCCI edits, ICD-10/CPT combos, modifier logic, LCD/NCD rules hardcoded over 15 years of payer policy changes | Denial spike at go-live; rules that were preventing denials stop functioning with no immediate error signal |
| Payer contract rate tables | Fee schedules, carve-outs, stop-loss thresholds often in flat-file databases disconnected from the billing engine | Systematic underpayment goes undetected for months; no automated comparison against contracted rates |
| Denial management workflows | Routing logic, appeal generation rules, timely filing tracking typically in stored procedures with no surface documentation | Automated denial workflows revert to manual; appeal windows missed |
| Charge capture rules | Service-to-CPT mapping, bundling and unbundling rules built by coding specialists responding to annual CPT updates | Missed charges and undercoding at the point of claim generation |
| Prior authorization routing | PA requirement triggers by payer, service type, and plan; payer-specific submission formats | CMS-0057-F non-compliance; 7-day clock violations; claims submitted without required PA |
| Remittance reconciliation | ERA/EOB parsing logic, contractual adjustment rules layered to accommodate each payer’s remittance format | Underpayments invisible without automated contract comparison |
| Clearinghouse integrations | Single-source EDI connections, payer-specific trading partner agreements | Single point of failure; no failover routing if the primary clearinghouse is disrupted |
The underpayment exposure is a particular blind spot. MGMA estimates that 7 to 11% of all claims are underpaid, a range that translates to millions of dollars annually for any health system processing meaningful claim volume.
One illustrative example: a 120-physician, 30-location practice recovered $10 million in underpayments after implementing automated contract management. The root cause was consistent with what appears across most legacy systems: actual payments were not being automatically compared against contracted rates because the contract rate logic was not surfaced in the billing system in a queryable form.
Claim scrubbing rules carry the highest immediate risk. A rule that migrates incorrectly does not produce an error message. It simply stops preventing a category of denials. The denial rate increases, and the connection to the migration takes weeks or months to establish, by which time revenue has already leaked through timely filing windows.
At 3 to 5% revenue leakage, legacy RCM technical debt carries a direct, measurable dollar cost. The adjudication rule extraction challenge is not unique to RCM; it mirrors the same problem in insurance claims processing, where rules accumulated over similar timelines produce identical migration risk.
These seven components accumulated the same way across every legacy billing system: built by billing specialists, not IT, added piecemeal with every payer policy change and coding update, never documented systematically. The result is a system that processes claims accurately until you try to move it.
Your billing system contains 15 years of claim scrubbing rules, payer contract logic, and denial workflows that nobody has fully mapped. Before any modernization path begins, that inventory needs to exist.
Legacyleap’s $0 Modernization Assessment delivers a complete dependency map, risk indicators, and modernization blueprint for your RCM codebase in 2 to 5 days, with no code leaving your environment.
Three RCM Modernization Paths: Replace, AI Overlay, or Comprehend First
Decision-makers evaluating RCM system modernization are typically weighing one of three paths. Each has a legitimate use case. Each has a failure mode that the components mapped in the previous section make entirely predictable.
Path 1: Full Platform Replacement
The US market for RCM platform replacement is well-developed, with established vendors covering the full revenue cycle. Implementation timelines for large health systems typically run 12 to 24 months, an extended transition during which the legacy system must remain operational and claim submission must continue without interruption.
The consistent failure mode is well-documented, though rarely discussed openly. Implementation teams configure new platforms from requirements documents and current-state interviews. If the health system cannot articulate what claim scrubbing rules exist in the legacy system, those rules either do not migrate or are approximated from vendor-standard templates. Most health systems cannot produce that inventory, for the reasons established in the previous sections.
The new platform goes live. Standard scrubbing rules apply. Denial rates increase because the payer-specific logic preventing those denials is no longer in place. Revenue cycle leadership spends months identifying missing rules, re-entering them, and recovering lost revenue while managing the timely filing clock on already-submitted claims.
Platform replacement succeeds when the health system can hand the implementation team a complete inventory of what the legacy system does. Without that inventory, it is a configuration exercise executed against incomplete information.
If your modernization program is already underway and claim scrubbing logic has not been inventoried, the risk is live. Book a Demo to see how Legacyleap extracts the complete financial logic catalog from a legacy RCM system before any migration step proceeds.
Path 2: AI Overlay on Legacy
A significant share of US healthcare organizations have taken a different approach, adding AI-powered RCM automation on top of the existing platform rather than replacing it. According to a 2024 HFMA/FinThrive survey, 63% of healthcare organizations have integrated AI-powered RCM automation, but only 15% have achieved positive ROI [6].
The ROI gap has a structural explanation. AI overlay adds pattern recognition and automation on top of the claim submission pipeline, but the underlying platform retains all the architectural fragility of the legacy core. A denial prediction model can flag that a claim is likely to be denied. It cannot fix the scrubbing rule generating the billing error, the payer contract table producing systematic underpayment, or the clearinghouse integration with no failover routing.
Adding intelligence to a system whose logic nobody has mapped does not make that logic visible. It makes the errors more anticipated, not more preventable.
Path 3: Comprehend-First Modernization
The third path is not a separate vendor category. It is a prerequisite discipline that determines whether either of the first two paths can succeed. Comprehend-first modernization begins by extracting the financial logic from the legacy system before any transformation begins: every claim scrubbing rule, every payer contract threshold, every denial routing condition, catalogued, attributed, and validated against actual billing behavior.
This inventory is what makes platform replacement safely configurable. It is what makes AI overlay reliably deployable. It is what allows a health system to hand an implementation team a complete specification rather than a partial one.
For building the budget case for RCM modernization investment, the comprehension phase is not overhead. It is risk mitigation with a direct dollar value, measured against the cost of a denial spike following an incomplete migration.
| Path | Prerequisite for Success | Failure Mode Without Comprehension | Timeline |
| Full platform replacement | Complete inventory of legacy billing logic to configure the new platform | Denial spike at go-live; months of post-launch remediation | 12 to 24 months |
| AI overlay on legacy | Stable, understood legacy logic for AI to operate against | Intelligence layered on top of unresolved architectural fragility | 3 to 9 months to deploy; ongoing ROI risk |
| Comprehend-first transformation | Extraction of all billing logic before any transformation begins | N/A; comprehension is the methodology | Variable; Assessment completes in 2 to 5 days, significantly dropping the overall timeline. |
How Legacyleap Modernizes RCM Systems: From Hidden Billing Logic to Validated, Deployment-Ready Platform
For US health systems evaluating modernization partners, the meaningful question is not which vendor offers the most automation. It is which service model addresses the specific risks that make RCM migration dangerous. Legacyleap’s five-agent workflow is structured around those risks. Each stage produces a concrete deliverable the health system owns, reviews, and acts on, and each one maps directly to a gap the preceding sections established.
Assessment Agent: What the System Actually Contains
In 2 to 5 days, you know exactly which claim scrubbing rules are undocumented, which clearinghouse integrations have no failover, and which components will produce a denial spike the moment you migrate them.
You get a complete dependency map of your RCM codebase, technical debt indicators, security vulnerability flags relevant to HIPAA compliance, and effort and timeline estimates grounded in the actual system.
That inventory is what every subsequent decision, whether to replace, overlay, or transform, depends on. No cost. No code leaves your environment.
Documentation Agent: The Financial Logic Catalog
After the Documentation Agent runs, your revenue cycle leadership can answer a question most health systems cannot: what claim scrubbing rules does your billing platform actually enforce?
Every rule, every payer-specific validation condition, every denial trigger, every PA routing requirement is extracted directly from source code and catalogued. Integration maps trace every clearinghouse dependency. Architecture diagrams show every module boundary and data flow.
This is the document that makes platform replacement safely configurable and AI overlay reliably deployable. It is what implementation teams have historically been asked to produce and have not had the tools to generate.
For HIPAA compliance, FHIR interoperability, and the broader clinical system context, this catalog also serves as the compliance traceability layer, a record of what the system does before any change is made.
Recommendation Agent: Migration Sequencing and Risk Scoring
Your modernization path is chosen based on what your system actually contains, not on a vendor relationship or a consultant’s approximation.
You get target framework selection grounded in actual system complexity, refactor-replace-retain decisions at the module level, and component-level risk scoring that tells you which areas require the most governance before cutover.
Migration phases are sequenced to protect cash flow continuity throughout the transition.
Modernization Agent: Governed, Diff-Based Transformation
Every code change surfaces as a reviewable pull request before any merge or deployment. No autonomous changes. No surprises in production.
Approximately 70% of modernization efforts are automated; the remainder is flagged explicitly for human review. The billing logic is transformed with full traceability from the original rule to the modernized equivalent, so your team can verify that the scrubbing rule that prevented a specific payer’s denial category still exists in the new system and still works.
QA Agent: Claim-for-Claim Parity Validation
Before any deployment proceeds, every claim scenario your legacy system handles is tested against the modernized platform. Auto-generated unit, integration, regression, and functional test cases cover the full billing workflow. Differential checks confirm identical billing outputs across the complete claim population. You go live knowing the migration is correct, not believing it.
This closes the gap between “we believe the migration is correct” and “we have verified it against the actual claim scenarios the system handles.”
For a system processing hundreds of millions in annual claims, that distinction is the difference between a controlled transition and a denial spike.
Deployment and Security Model
All analysis and transformation occur inside the client’s infrastructure. Source code is processed on-premise or within a client-controlled VPC. No RCM billing logic, payer contract data, or patient-associated financial information touches an external system. Scheduling is the front door of the revenue cycle, where insurance verification begins at patient access, and the full pipeline remains within the client’s security boundary throughout the engagement.
For US health systems operating under HIPAA and cyber insurance requirements, this deployment model eliminates the data governance risk that external processing would create. Effort savings across the modernization lifecycle run 40 to 50%, with potential for up to 70% depending on stack complexity and scope.
Modernize the System That Processes Every Dollar of Your Revenue
The $48.4 billion in revenue leakage across US hospitals in 2025 is the aggregate cost of billing platforms processing every dollar of revenue without anyone fully knowing what rules they run. Payer AI is accelerating the denial rate. CMS-0057-F is in effect.
FHIR API compliance requires architectural changes by January 2027. The Change Healthcare architecture lesson applies to every health system still running a centralized, single-source billing infrastructure.
Every modernization path requires the same prerequisite: an inventory of what the billing system actually does, extracted before any change is made. Without it, platform configuration is guesswork, AI automation operates against an unstable foundation, and go-live is a calculated risk rather than a verified deployment.
If you are still evaluating whether RCM modernization is the right program to fund, start here. Legacyleap’s $0 Assessment delivers the dependency map, risk indicators, modernization blueprint, and effort estimates your decision requires. In 2 to 5 days, you have an evidence-based view of what your legacy billing platform contains and what it will take to modernize it safely. No cost. No code leaves your environment.
If you know modernization is needed and want to see exactly how the agent workflow operates against a legacy RCM system, from financial logic extraction through claim-for-claim parity validation, book a Demo.
FAQs
Denial spikes after go-live are not a temporary adjustment. Claims already submitted during the window between go-live and error detection are subject to timely filing deadlines, typically 60 to 365 days depending on payer contract. Revenue that misses that window cannot be recovered through appeals or resubmission. For a $500M health system running at 1.3% operating margin, a 2 to 3 percentage point increase in denial rate in the weeks following launch can permanently eliminate several million dollars in revenue.
Claim scrubbing rules carry the highest risk because they fail silently. When a scrubbing rule does not migrate correctly, it does not generate an error. It simply stops preventing a category of denials. Payer contract rate tables are the second highest risk, because underpayment resulting from missing contract logic accumulates undetected for months. Both components share the same root cause: they were built by billing specialists rather than IT, and were never formally documented.
CMS-0057-F requires payers to issue standard prior authorization decisions within 7 calendar days, effective January 1, 2026, with full FHIR API compliance required by January 2027. Legacy RCM systems built without real-time PA tracking cannot meet these timelines without architectural changes. Health systems running legacy platforms face two risks: regulatory non-compliance and claims submitted without required PA, both of which produce denials that cannot be recovered once timely filing windows close.
Validation requires systematic claim-for-claim parity testing between the legacy system and the modernized platform, not spot checks or sampled testing. Every claim scenario the legacy system handles needs to produce an identical billing output in the modernized equivalent before any go-live proceeds. This means auto-generated test cases covering the full billing workflow, including edge cases in payer-specific scrubbing rules and contract rate calculations, with differential checks confirming output parity across the complete claim population.
Timeline depends on platform complexity and the modernization path chosen. Full platform replacement for large US health systems typically runs 12 to 24 months, with the legacy system remaining live throughout. The prerequisite step, extracting and cataloguing all billing logic before any migration begins, adds 2 to 5 days for the assessment phase and several weeks for full documentation of complex legacy codebases. Skipping that step does not save time. It relocates the time cost to post-launch remediation, where it is significantly more expensive.
References
[1] Kodiak Solutions. State of the Healthcare Revenue Cycle. Business Wire, March 31, 2026. Dataset from 2,300 US hospitals covering full-year 2025 denial rates and net revenue leakage figures. https://businesswire.com/news/home/20260331038554/en/Healthcare-Provider-Organizations-Saw-Net-Revenue-Losses-From-Final-Denials-and-Bad-Debt-Grow-by-25-in-2025-According-to-Kodiak-Solutions-Proprietary-Data
[2] Kaufman Hall. National Hospital Flash Report: December 2025 Hospital Financial, Volume and Margin Trends. Kaufman Hall, December 2025. Adjusted year-to-date operating margin data from 1,300+ US hospitals. https://www.kaufmanhall.com/insights/research-report/national-hospital-flash-report-december-2025-data
[3] Raza, S., Gerke, S., Silcox, C. et al. “Medicare Advantage Becoming a Disadvantage with Use of Artificial Intelligence in Prior Authorization Review.” npj Digital Medicine, February 4, 2026. https://www.nature.com/articles/s41746-026-02387-x
[4] Centers for Medicare & Medicaid Services. CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F). CMS.gov, effective January 1, 2026. FHIR API compliance deadline: January 1, 2027. https://www.cms.gov/newsroom/fact-sheets/cms-interoperability-prior-authorization-final-rule-cms-0057-f
[5] American Medical Association. “Physicians Struggle to Keep Practices Afloat After Change Cyberattack.” AMA Press Release, April 10, 2024. Survey data: 80% of physician practices reported lost revenue; $8.9B in emergency advances required. https://www.ama-assn.org/press-center/ama-press-releases/physicians-struggle-keep-practices-afloat-after-change-cyberattack
[6] HFMA and FinThrive. “Most Healthcare Organizations Are Adopting AI in the Revenue Cycle.” HFMA, 2024 survey of 101 healthcare organizations. Vendor-sponsored. https://www.hfma.org/technology/most-healthcare-organizations-are-adopting-ai-in-the-revenue-cycle-hfma-poll/